
10-Year Commitment to Global Health and Rights: Annual Report for 2021-2022
ISSN #: 2817-2159
This report reviews the second year of implementation of the Government of Canada’s 10-year commitment to global health and rights (10YC). It focuses on our spending, policy and programming efforts and results from April 1, 2021, to March 31, 2022.
On this page:
- I. Executive summary
- II. Introduction
- III. 2021-2022: 10YC year in review
- IV. Making progress on the 10YC
- V. COVID-19 response and recovery
- VI. Transparency, engagement and learning
- VII. Looking forward
- Annex I – Adjusted 2020-2021 spending totals
- Annex II – Key multilateral results
I. Executive summary
Canada’s 10-Year Commitment to Global Health and Rights (10YC) builds on over 2 decades of leadership in global health. It represents the government’s largest and longest sectoral commitment in international development assistance. The 10YC is a key vehicle for us to deliver on the objectives of the 2030 Agenda for Sustainable Development and builds on our historical and current leadership in global health and nutrition. The report constitutes a milestone under our Accountability Framework for the 10YC, ensuring transparent and timely information on how investments are improving health outcomes. This report provides a financial summary of the second year of implementation between April 1, 2021, and March 31, 2022. It also highlights key programming, policy and advocacy results achieved in:
- global health
- comprehensive sexual and reproductive health and rights (SRHR)
- gender-sensitive nutrition
The 2021-2022 10YC report shows that we are continuing to ramp up our spending to meet the target of an average of $1.4 billion annually by 2023-2024 as planned, including $700 million for SRHR each year. In 2021-2022, our 10YC funding continued to protect country investments in global health from COVID-19 pandemic repercussions. This includes investments in essential health services, infectious disease prevention, SRHR and nutrition. Highlights include:
- $1.278 billion in total global health investments in 2021-2022 under the 10YC—a 2% increase from the previous year—delivered through nearly 605 projects with over 366 partners.
- A 14% increase in SRHR programming investment, with $567.49 million invested as compared to $496 million in 2020-2021.
- $208.2 million invested in overall SRHR neglected area programming, representing an increase of 22% from $170.9 million in 2020-2021. Investments increased in all 5 neglected areas, reflecting the increased ability of the department to capture neglected area spending in 3 areas previously captured under more general reproductive health services.
- In line with the Feminist International Assistance Policy (FIAP), 65% of bilateral and multilateral health investments were directed to the sub-Saharan African region. Of the top 10 country recipients of 10YC funding, 8 were in sub-Saharan Africa.
- The COVID-19 pandemic remained a significant challenge in 2021-2022. We disbursed a one-time additional $465 million (not included under the 10YC) in 2021-2022. This helped us continue to play a leadership role in the COVID-19 global response to ensure equitable global access to vaccines, treatments and diagnostics.
- In 2021-2022, our Minister of International Development continued to play an important advocacy role to advance FIAP and our global health priorities with stakeholders and in global fora.
At the first 10YC stakeholder workshop in February 2023, partners provided feedback on the first 10YC report for 2020-2021. In line with the 10YC Accountability Framework, this report incorporates the valuable feedback received. It provides examples of results achieved across the full spectrum of the global health portfolio, including Canada’s governance role on boards of key multilateral global health partners.
The increase in global health investments in 2021-2022, particularly in SRHR, reflects the government’s continued dedication to improving health outcomes and to addressing critical gaps in the global health landscape.
II. Introduction
In June 2019, Canada announced the 10-Year Commitment (10YC)Footnote 1 to increase global health funding between 2020 and 2030 to reach an average of $1.4 billion annually by 2023-2024. Of this, the 10YC pledges an average of $700 million per year for sexual and reproductive health and rights (SRHR), with a particular focus on the following neglected or underfunded areas of SRHR:
- safe abortion and post-abortion care
- comprehensive sexuality education (CSE)
- family planning and contraception
- SRHR advocacy and reform
- prevention of and response to sexual and gender-based violence (SGBV)
The 10YC is our longest and largest sectoral financial commitment for international development assistance and represents a key commitment under the Feminist International Assistance Policy (FIAP) to advance the health and rights of women and girls.
The 10YC is a key funding initiative for us to deliver on the 2030 Sustainable Development Goals (SDG)—primarily SDG 3 (Good Health and Well-Being) and SDG 2 (Zero Hunger). It also contributes to SDG 5 (Gender Equality), SDG 6 (Clean Water and Sanitation), SDG 10 (Reduced Inequalities) and SDG 16 (Peace, Justice and Strong Institutions). The 10YC builds on our long-standing partnerships with multilateral, bilateral and civil society organizations (CSOs) in the health and nutrition sector and follows 3 Canadian legacy global health initiatives:
- 2010 to 2015: $2.85 billion Muskoka Initiative for Maternal, Newborn and Child Health (MNCH)
- 2016 to 2020: $3.5 billion renewed MNCH Initiative
- 2017 to 2020: $650 million Her Voice, Her Choice Commitment
SRHR is a key investment and leadership area under the 10YC. In addition to SRHR, we are continuing to focus on global infectious disease prevention and control and on maternal and child health and nutrition. We are a long-standing supporter of key global health partners in these areas, including the Global Fund to Fight AIDS! and Malaria, Gavi, the Vaccine Alliance, the Global Financing Facility for Women, Child and Adolescent Health, the Global Polio Eradication Initiative, the World Health Organization, UNFPA, UNICEF, UNAIDS, the Stop TB Partnership, and Nutrition International.
The 10YC is supported by an Accountability Framework developed with Canadian and international stakeholders. As part of the Accountability Framework, Global Affairs Canada (GAC) publishes this annual report to document progress under the 10YC. GAC convenes an annual stakeholder workshop each fall to discuss and inform future programming and advocacy efforts. This year’s report takes into consideration feedback from partners on the first 10YC report provided at the first stakeholder workshop in February 2023—namely, to provide more information on results achieved across the full health and nutrition portfolio and to offer more visibility on how FIAP and 10YC priorities are implemented through our multilateral investments.
From the start of the commitment in 2020 to 2022, we have ramped up global health investments toward the announced target of an average of $1.4 billion by 2023-2024. The 2020-2021 10YC report showed a baseline expenditure of $1.25 billion for the commitment, including $755 million for health and nutrition and $496 million for SRHR investments between April 1, 2021, and March 31, 2022.
This report demonstrates our increased expenditure and highlights results achieved through advocacy, policy and programming efforts between April 1, 2021, and March 31, 2022.
III. 2021-2022: 10YC year in review
10YC financial reporting update
The primary sources of funding for the 10YC are Global Affairs Canada’s (GAC) development international assistance (including contributions to international financial institutions), the international assistance portion of GAC’s assessed WHO contribution for health, Finance Canada’s international assistance support to the World Bank International Development Association and Canada’s International Development Research Centre’s (IDRC) international assistance expenditures in global health and SRHRFootnote 2. Adjusted figures for 2020-2021 consistent with these sources of funding can be found in Annex 1.
10YC investments are tracked thematically using GAC’s 10YC coding methodology. The 10YC coding methodology uses Canada’s sector codes. These codes are based on the Organisation for Economic Co-operation and Development (OECD) Development Assistance Committee (DAC) purpose codes, the global standard used by bilateral donors, including Canada.
Canada’s overall international assistance spending, including sources of spending beyond what is counted in the 10YC, is published in the Canada’s International Assistance Data, as per the Official Development Assistance Accountability Act.
Ramping up 10YC spending
In 2021-2022, total investments under the 10YC amounted to $1.278 billion, an increase of $27.1 million (or 2%) from 2020-2021. Reaching the $700 million SRHR investment target means rebalancing our global health investments toward SRHR programming. Of the $1.278 billion invested this year, $567.49 million was invested in SRHR—an increase of $71.61 million (or 14%) from the previous year. Our spending on other global health programming totalled $710.51 million.
Our funding for the COVID-19 crisis in 2020 and 2021 led to a strong and swift response to the pandemic while also playing an important role in protecting country investments in global health from COVID-19 pandemic repercussions (i.e., basic health service provision, infectious disease prevention, SRHR and nutrition). A significant part of GAC’s COVID-19 international assistance response was delivered through one-time additional funding to the department outside of the 10YC funding. As the global response to COVID-19 shifted from acute response to recovery, prevention, and preparedness for future health emergencies in 2021-2022, our new COVID-19 health funding (outside the 10YC) was scaled down by 57%, from $1.086 billion (2020-2021) to $465 million (2021-2022).
Figure 1: Global health and SRHR spending before and during the 10YC

Text version
- 2017-2018
- Global health: $1.2B
- SRHR: $0.370B
- 2018-2019
- Global health: $1.2B
- SRHR: $0.416B
- 2019-2020
- Global health: $1.2B
- SRHR: $0.447B
- 2020-2021 (10YC)
- Global health: $1.3B
- SRHR: $0.496B
- Global health (including additional COVID-19 response funding): $2.3B
- SRHR (including additional COVID-19 response funding): $0.549B
- 2021-2022 (10YC)
- Global health: $1.3B
- SRHR: $0.567B
- Global health (including additional COVID-19 response funding): $1.7B
- SRHR (including additional COVID-19 response funding): $0.567B
- 2023-2024 (10YC target)
- Global health: $1.4B
- SRHR: $0.700B
10YC investments by region
A regional breakdown of global health investments shows that the majority of bilateral and multilateral investments were directed to the sub-Saharan Africa region (65%). This directly contributes to the FIAP target of directing 50% of all of Canada’s international assistance to the region.
Figure 2: 10YC investments by geographical region
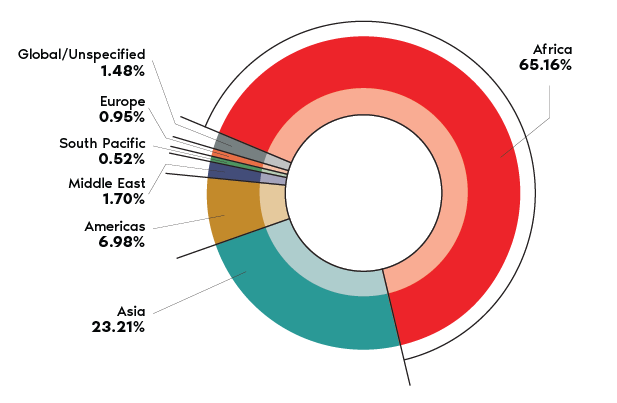
Text version
- Africa: 65.16%
- Asia: 23.21%
- Americas: 6.98%
- Middle East: 1.70%
- South Pacific: 0.52%
- Europe: 0.95%
- Global/Unspecified: 1.48%
In 2021-2022, 8 of the top 10 country recipients were in sub-Saharan Africa.
Figure 3: Top 10 country recipients of 10YC funding
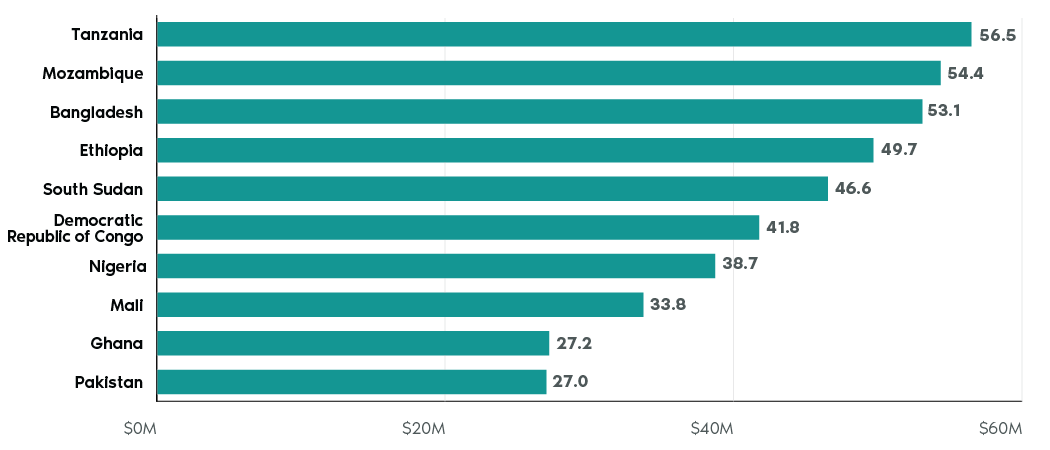
Text version
- Tanzania: $56.5M
- Mozambique: $54.4M
- Bangladesh: $53.1M
- Ethiopia: $49.7M
- South Sudan: $46.6M
- Democratic Republic of Congo: $41.8M
- Nigeria: $38.7M
- Mali: $33.8M
- Ghana: $27.2M
- Pakistan: $27.0M
10YC investments by partner type
We deliver on the 10YC through support to multilateral and global health platforms, as well as through direct partnerships with governments and Canadian, international, and local CSOs. In 2021-2022, the 10YC was delivered through nearly 605 projects with 366 partners. The Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund) received the most funding under the 10YC, while the top 10 recipients of 10YC funding included a mix of multilateral, SRHR, nutrition, and Canadian CSO partners.
Figure 4: Top 10 partners funded under the 10YC
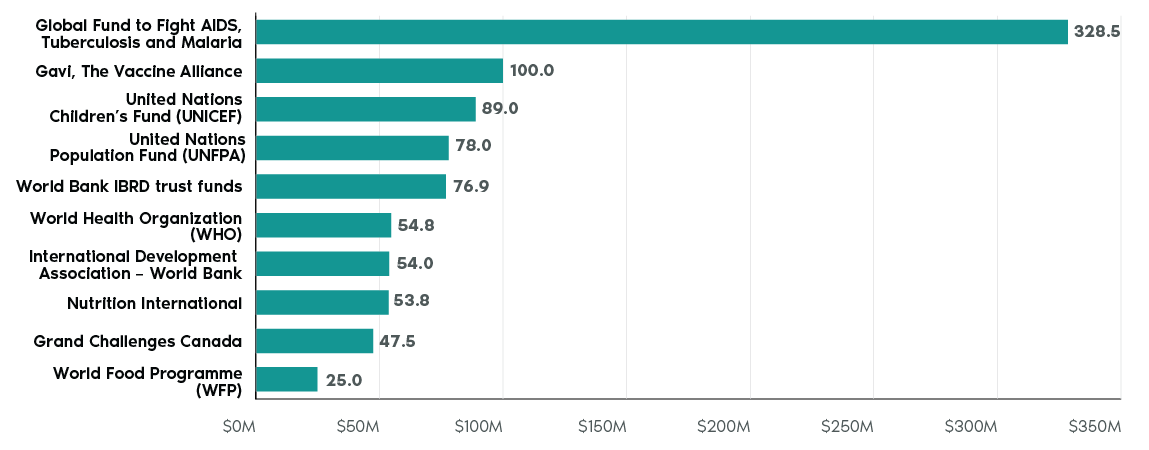
Text version
- Global Fund to Fight AIDS, Tuberculosis and Malaria: $328.5M
- Gavi, the Vaccine Alliance: $100.0M
- United Nations Children’s Fund (UNICEF): $89,0M
- United Nations Population Fund (UNFPA): $78,0M
- World Bank IBRD trust funds: $76.9M
- World Health Organization (WHO): $54.8M
- International Development Association: $54,0M
- Nutrition International: $53.8M
- Grand Challenges Canada: $47.5M
- World Food Programme (WFP): $25,0M
In 2021-2022, the majority of funding was channelled through multilateral organizations (69.6%), with a significant amount channelled through CSOs (26.8%).
Figure 5: Percentage of 10YC funding by partner type
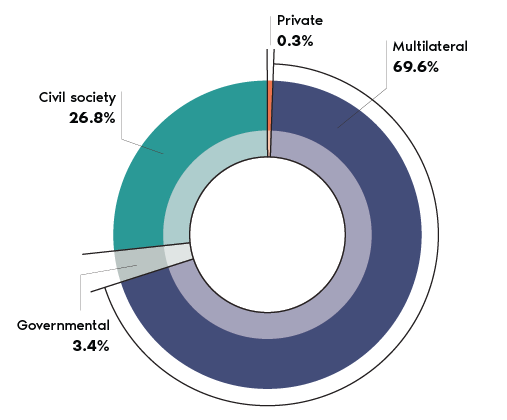
Text version
- Multilateral: 69.6%
- Civil society: 26.8%
- Governmental: 3.4%
- Other: 0.3%
Key multilateral investments
Within the global health sector, Canada is a board member at the Global Fund, Gavi the Vaccine Alliance (Gavi), Nutrition International, the Global Financing Facility for Women, Child and Adolescent Health (the GFF), UNICEF, UNFPA, UNAIDS the Global Polio Eradication Initiative (the GPEI) and the Stop TB Partnership. Our investments contribute to the overall results achieved by these organizations, and we also play a key role as a board member in the governance and reporting provided by these partners. Our funding and influence ensure that Canadian priorities for advancing gender equality, nutrition and SRHR are reflected in organizational priorities and structures. A description of key multilateral results and Canada’s influence on these boards in 2021-2022 can be found in Annex II.
Measuring the 10YC through key performance indicators
10YC performance is measured in part through a set of key performance indicators (KPIs) for health and nutrition, in line with the FIAP Human Dignity Action Area. The KPIs provide us with an important subset of annually collected data for projects where GAC is the sole donor and implementing organizations report on the number of people reached as a direct result of our 10YC spending. However, the KPI data does not capture the full reach of our investments in health and nutrition. It does not include data from investments through multilateral organizations, initiatives with multiple donors, or direct budget support to governments.
In 2021-2022, based on GAC’s project KPI dataFootnote 3, GAC funding reached over 12 million people through more than 70 projects globally, an increase from 10 million people reached in 2020-2021.
Throughout the report, KPI Data Spotlight insets have been included to highlight how this subset of investments under the 10YC has reached beneficiaries.
KPI data spotlight: People reached through health services and programs
Figure 6: KPI data: People reached through health services and programs
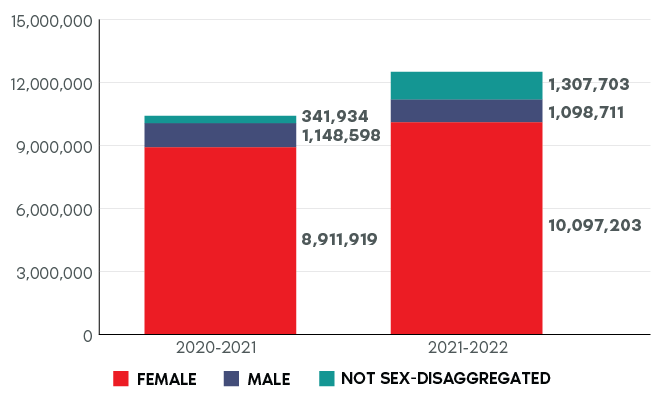
Text version
- Males 2020-2021: 1,148,598
- Females 2020-2021: 8,911,919
- Not sex-disaggregated: 2020-2021: 341,934
- Males 2021-2022: 1,098,711
- Females 2021-2022: 10,097,203
- Not sex-disaggregated 2021-2022: 1,307,703
Not sex-disaggregated refers to data not broken down by sex.
IV. Making progress on the 10YC
Global health
In 2021-2022, the COVID-19 pandemic continued to strain national economies, supply chains and access to essential social and health services. This stress on health systems led to the largest backslide in access to child vaccinations in over 3 decades. To offset the impact of the pandemic and as part of 10YC and COVID-19 funding, in 2021-2022, we supported partners to maintain their programming for essential health services, such as access to sexual and reproductive services; routine maternal, newborn and child vaccinations; and micronutrient supplements and nutritious food.
The COVID-19 pandemic resulted in a steep decline in the availability and accessibility of crucial medical supplies, including medications for diseases like malaria and tuberculosis. It also caused disruptions to supply chains, hindering access to nutritious food and essential micronutrient supplements. The pandemic’s devastating health and socio-economic impacts highlighted the complex interconnectedness of global health systems and underscored the need for investments in equitable and resilient health systems that provide essential health services to the most marginalized and contain outbreaks before they become pandemics.
KPI data spotlight: Women reached with maternal and newborn health services
Between 2020-2021 and 2021-2022, KPI data shows that women reached with maternal and newborn health services increased due to investments in essential health services as part of our COVID-19 response.
Figure 7: KPI data: Women reached with maternal and newborn health services
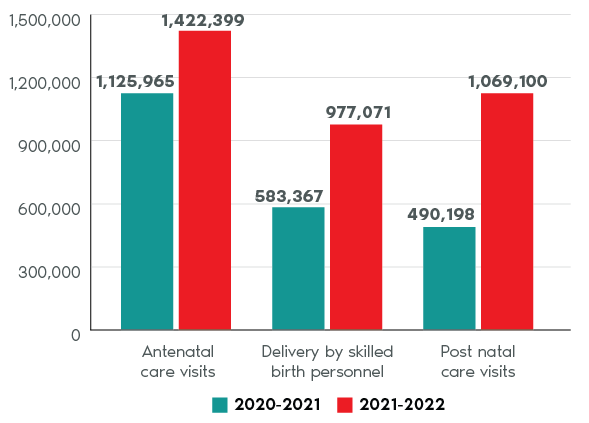
Text version
- Antenatal care visits 2020-2021: 1,125,965
- Antenatal care visits 2021-2022: 1,422,399
- Delivery by skilled birth personnel 2020-2021: 583,367
- Delivery by skilled birth personnel 2021-2022: 977,071
- Postnatal care visits 2020-2021: 490,198
- Postnatal care visits 2021-2022: 1,069,100
Conversely, the KPI data showed that there was a drop in community-based health services between 2020-2021 and 2021-2022, from approximately 1.5 million people to just over 250,000. This is likely because partners experienced community-based programming disruptions. Data collection and reporting by partners was also significantly disrupted due to COVID-19 restrictions between 2020 and 2022.
Delivery of health services: 5 key global health partnerships for Canada in 2021-2022
In 2021-2022, we made large investments in multilateral health partners to continue expanding the delivery of essential health services. Below are highlights of results from a selection of key partners (the Global Fund, Gavi, the GPEI, the GFF and the Stop TB Partnership’s TB REACH initiative), which represent a subset of the broader work that GAC supports in global health.
Project spotlight: Global Fund
We committed $930.4 million for the 2020-2021 to 2022-2023 period to support the lifesaving work of the Global Fund, which has resulted in over 44 million lives saved. In 2020 (the most recent year for which data is available), the Global Fund provided access to antiretroviral therapy for 21.9 million people living with HIV, treated 4.7 million people with TB and distributed 188 million mosquito nets. Through our COVID-19 response funding in 2021-2022 and as a core partner of the Access to COVID-19 tools Accelerator (ACT-A), Canada also provided $125 million to support the Global Fund’s contribution to the COVID-19 response. The Global Fund helped low and middle-income countries strengthen health systems and access tests, treatments (including medical oxygen) and personal protective equipment.
Gavi: We have committed $600 million to Gavi, the Vaccine Alliance, for its 2021 to 2025 strategic period. As of 2020 (the most recent year for which data is available), our funding has helped Gavi to immunize more than 888 million children, helping to prevent more than 15 million deaths. Gavi aims to reach an additional 300 million by the end of 2025. As a result of the pandemic, some countries experienced backsliding of immunization coverage in 2020. In 2021, with direction from the Gavi Board (which we are a member of), Gavi began to focus on helping countries to maintain, restore and strengthen immunization services. This included campaigns to catch up on missed immunizations and to introduce new vaccines into routine immunization programs.
Global Polio Eradication Initiative: In 2021-2022, we provided $56.5 million to the Global Polio Eradication Initiative (GPEI). This included $34.5 million for the World Health Organization and $22 million for UNICEF. In 2021, our contributions helped the GPEI vaccinate more than 370 million children multiple times in 30 countries with over one billion doses of oral polio vaccine. Our support also helped the GPEI respond to outbreaks in the endemic countries of Afghanistan and Pakistan, along with several other countries across Africa and Asia. The GPEI also strengthened surveillance systems and supported COVID-19 responses.
Global Financing Facility: In 2021-2022, we provided $50 million in institutional support, and on June 30, 2021, we committed an additional $50 million to the GFF’s Essential Health Services (EHS) grants. This funding has supported access to reproductive, maternal and child health services in 36 countries, improving health systems, mitigating the impact of COVID-19 and driving long-term improvements for women, children and adolescents. Our support through the GFF also serves to catalyze significant additional financing from the World Bank’s International Development Assistance and other funding sources for health interventions for women, children and adolescents; for country-led development; and ultimately, for advancing the Sustainable Development Goals.
Stop TB Partnership’s TB REACH initiative: We provided $85 million to the TB REACH initiative for the 2016-2021 period. Over the last decade, 330 TB REACH projects in 56 countries have enabled the screening of more than 42 million people, the detection and treatment of more than 2.8 million people with TB, and the prevention of more than 15 million infections, saving almost 1.5 million lives. Interventions initiated by TB REACH have been scaled up in many different countries and settings, leveraging more than $200 million in support from other donors. While we provide foundational support for TB REACH, other donors including the U.S., the U.K., the Bill and Melinda Gates Foundation and Unitaid have also contributed more than $45 million to the TB REACH initiative.
Delivery of health services: Country-specific examples in 2021-2022
Bangladesh: With support from Canada, the International Centre for Diarrhoeal Disease Research in Bangladesh provided treatment to more than 200,000 patients. Our support also enabled the Dhaka Hospital to treat 209,353 patients during diarrhoeal outbreaks in Dhaka and in many other parts of the country.
Maldives: With our support, the Sanitization of Health Care Waste in COVID-19 Management Sites project worked to reduce the transmission risk of COVID-19 and other infectious diseases in the Maldives by providing key equipment and facilities in 40 islands, as well as assessments of 37 health facilities. In addition, the Ministry of Health developed and endorsed national standards for waste handling.
Venezuela: Through the Integrating Venezuelan Health Professionals project in Peru, our support to UNHCR helped 731 Venezuelan health professionals—including doctors, psychologists, and nurses—to validate their professional degrees and their registration in professional boards. At least 50% of selected health professionals were women.
Sexual and reproductive health and rights
Having support for sexual and reproductive health and rights (SRHR) means that all individuals have the rights, knowledge and means to make decisions and access services concerning their reproductive lives and sexuality without facing criminalization, coercion, discrimination or violence. Canada takes a comprehensive approach to advancing SRHR, in line with the Guttmacher Lancet-Commission report. This means we work to:
- support the provision of an essential SRHR intervention package based on a life-course approach
- apply equity in access to, and quality of, care without discrimination and with accountability
- meet and respond to SRHR needs and issues through services, education, counselling and information
- address gendered inequalities, discriminatory social norms and institutional structures that limit the attainment of SRHR
The 10YC’s focus on comprehensive SRHR, including the neglected areas, is unique among donors and critically important to protect the rights of women and girls to bodily autonomy and sexual and reproductive health services.
In 2021-2022, we increased our programming in SRHR to $567.49 million from the baseline expenditure of $496 million in 2020-2021, a $71.61-million or 14% increase. There was a continued focus on the SRHR neglected or underfunded areas of:
- safe abortion and post-abortion care
- comprehensive sexuality education (CSE)
- family planning and contraception
- SRHR advocacy and reform
- prevention of and response to sexual and gender-based violence (SGBV)
Project spotlight: Grand Challenges Canada in sub-Saharan Africa
In 2021-2022, Grand Challenges Canada (GCC) committed $15.9 million to funding 56 innovations in 33 countries to address challenges in humanitarian settings, maternal, newborn and child health, early childhood development, mental health, sanitation, SRHR, and safe abortion. For example, GCC is supporting transition to scale of South African medical device manufacturer Sinapi Biomedical Limited’s Ellavi Uterine Balloon Tamponade, which has been specifically designed to treat postpartum hemorrhage in low-resource health facilities. As of March 2022, this technology has saved the lives of over 2,800 women and improved the lives of a further 12,000 women in sub-Saharan Africa.
KPI data spotlight: People reached with sexual and reproductive health and family planning services and programs
KPI data shows that there was an increase in the number of people reached across all sexual and reproductive health services between 2020-2021 and 2021-2022. Despite decreased access to sexual and reproductive health services due to COVID-19 restrictions, GAC-funded partners scaled up efforts and were able to directly support continuity of lifesaving sexual and reproductive health services in nearly 30 countries.
Figure 8: KPI data: People reached with sexual and reproductive health services and programs.
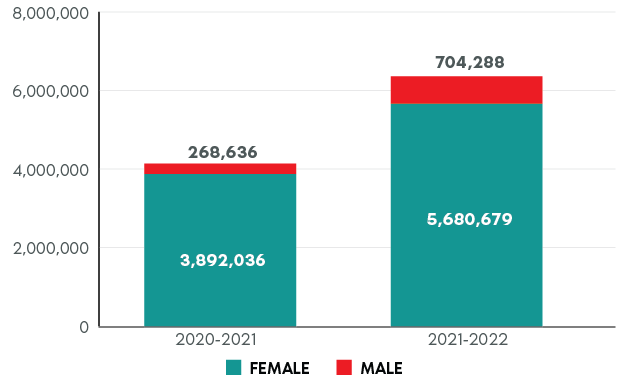
Text version
- Male 2020-2021: 268,636
- Female 2020-2021: 3,892,036
- Male 2021-2022: 704,288
- Female 2021-2021: 5,680,679
SRHR neglected areas
In 2021-2022, there was an increase of 22% in overall SRHR neglected area investments, with $208.2 million invested compared to $170.9 million in 2020-2021. Investments increased in all 5 areas. The implementation of GAC-specific sector coding increased the ability of the department to capture neglected area spending in SRHR advocacy and reform, CSE, and safe abortion services and post-abortion care, which were previously captured under more general reproductive health services. Family planning saw the largest overall increase in spending, with a total increase of $15.9 million.
Figure 9: Sexual and reproductive health and rights neglected areas spending under 10YC
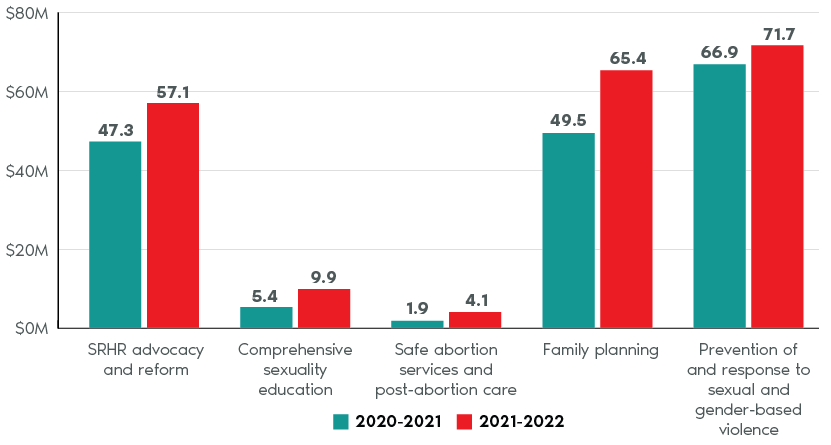
Text version
- SRHR advocacy and reform
- 2020-2021: $47.3M
- 2021-2022: $57.1M
- Comprehensive sexuality education
- 2020-2021: $5.4M
- 2021-2022: $9.9M
- Safe abortion services and post-abortion care
- 2020-2021: $1.9M
- 2021-2022: $4.1M
- Family planning
- 2020-2021: $49.5M
- 2021-2022: $65.4M
- Prevention of and response to sexual and gender-based violence
- 2020-2021: $66.9M
- 2021-2022: $71.7M
Programming by SRHR neglected area
In the face of rising opposition movements, it remained a challenge to ramp up programming in the neglected areas in some contexts in 2021-2022, particularly safe abortion services and post-abortion care and CSE. Not all partners have the capacity to focus on the neglected areas and existing partnership mechanisms for increasing abortion and CSE programming are at a smaller scale. Nevertheless, we are committed to seeking opportunities to increase investments in all the neglected areas as demonstrated in the following section.
Safe abortion and post-abortion care
Evidence shows that abortion restrictions force women to turn to unregulated and unsafe methods that cause injury and death. An estimated 25 million unsafe abortions take place every year (45% of all abortions), with 97% of these taking place in developing countries, where 220 women die from every 100,000 unsafe abortions.
The international non-governmental organization Ipas used Canadian funding in 2021-2022 to develop innovative tools, train hundreds of front-line workers, pilot innovative approaches to safe provision of medical abortion and launch a telehealth model to provide consultations and referrals at the community level. In Bangladesh, our funding helped Ipas to partner with the national telemedicine service, Shastho Batayon, to incorporate medical abortion, post-abortion care and contraceptive services into existing services. As of December 2020, this specific initiative trained 94 medical officers, 20 non-medical call centre agents and 5 medical officers, in addition to supporting the finalization of an SMS-based prescription system.
Comprehensive sexuality education
While many countries have policies, laws and frameworks in place for CSE, implementation for children and adolescents both in and out of school is uneven and often faces challenges resulting from issues related to jurisdiction over education, inadequate training for teachers and opposition to or misinformation about the content or impact of CSE, and a lack of understanding of the benefits of CSE.
Project spotlight: Project Brave in Columbia
Project Brave: Rights for Girls through SRHR Education, funded by Canada and implemented by the leading Colombian non-profit Profamilia, delivered a comprehensive sexuality education model in 8 municipalities of Colombia, where children and adolescents—along with their families, communities and local government institutions—are demonstrating significant changes in their SRHR knowledge, attitudes and practices. In 2021-2022, Brave worked with 10,361 adolescents (51% women and 49% men). The project also worked with their families, 376 teachers and 63 public servants and health officials on adolescent and youth-friendly health services and the incorporation of a gender and rights approach to public policy implementation and referral pathways for gender-based violence. By March 2022, 43% of schools had designed or updated their Sexuality Education and Citizenship Program with support from the project. By March 2022, children and youth were demonstrating the most significant changes. Girls, boys and adolescents are questioning and challenging unequal and discriminatory practices and have begun researching and designing initiatives to address the issues that matter to them in their lives, families, schools and communities.
In 2021-2022, the Canadian-funded Rights from the Start project was implemented by Action Canada in Bolivia, Ecuador, Guyana and Peru, reaching 52,740 adolescent girls and boys with CSE that incorporates innovative and youth-friendly virtual tools. We also worked with Plan International Canada in Bolivia to empower young girls and boys as allies in reducing teenage pregnancy and early marriage through CSE. Through Plan’s ARRIBA project, young women and men lead the discussion on CSE in their communities to promote sexual and reproductive rights and to raise awareness about denouncing acts of rape and child marriage as a strategy to escape poverty. The project reached over 4,500 adolescents (56% of whom were young women) through peer-to-peer education and training of over 2,100 traditional leaders 58% of whom were women.
Family planning and contraception
During the COVID-19 pandemic in 2021-2022, we made strategic investments to support and maintain access to family planning services and contraception for women and girls despite the lockdowns and other barriers. Our multilateral and bilateral investments in UNFPA (including UNFPA Supplies) in 2021-2022 enabled continued access to family planning commodities by women and adolescent girls in countries such as Burkina Faso, Ghana, Mali, Pakistan and Tanzania.
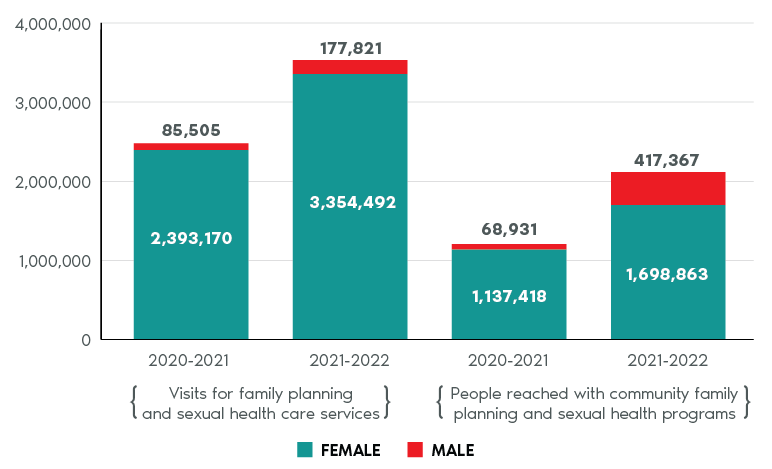
KPI data spotlight: People reached with family planning and sexual health care services and programs
Figure 10: KPI data: People reached with family planning and sexual health care services and programs
Text version
Visits for family planning and sexual health care services
- Male 2020-2021: 85,505
- Female 2020-2021: 2,393,170
- Male 2021-2022: 177,821
- Female 2021-2022: 3,354,492
People reached with community family planning and sexual health programs
- Male 2020-2021: 68,931
- Female 2020-2021: 1,137,418
- Male 2021-2022: 417,367
- Female 2021-2022: 1,698,863
Through over $15 million in bilateral and multilateral support to UNFPA in 2021-2022, we contributed to restoring many programs and services that were disabled during the pandemic. During this period, 74% of UNFPA program countries were able to maintain or expand family planning services at the community level, reaching 116 million women and young people with sexual and reproductive health services.
In Pakistan, we supported a UNFPA project that helped enable women, adolescents, and youth to exercise their reproductive rights without facing coercion, discrimination or violence. In 2021, the project refurbished 12 public health facilities in 2 districts of Sindh, trained 3,333 health care providers on family planning approaches and provided 1.2 million men and women with family planning services, including over 85, 000 individuals who accessed the services for the first time.
Through the UNFPA project Promoting the Sexual and Reproductive Rights of Adolescents in Honduras (DEREJUV), we supported 32 public health facilities in the provision of more adolescent-friendly integrated sexual and reproductive health services for over 280,000 adolescents. Strategic partnerships were developed with 7 institutions, including the Ministry of Health, the Ministry of Education and the Honduran Association of Municipalities. This has improved the coordination of efforts between key stakeholders supporting the prevention of adolescent pregnancies at local and national levels.
In 2021-2022, we also supported Partners in Health Canada through the No Woman or Girl Left Behind project to improve the provision of gender-sensitive and rights-based sexual and reproductive health services for adolescents. This project reached over 1,400 adolescent girls aged 10 to 19 in Malawi and over 2,000 adolescent girls in Sierra Leone, providing access to contraception and counselling services. The Adolescent and Youth-Friendly Services clinic in Sierra Leone also recorded over 3,500 visits in 2021-2022 with our support, a significant increase over the previous year. We also supported Humanity & Inclusion Canada in reaching over 30,000 adolescent girls and boys with SRH services and contraception in Côte d'Ivoire, Senegal and Togo.
Project spotlight: Family planning in the Philippines
In the Philippines, we are funding Oxfam Canada to work with local governments and CSOs to empower women and girls to exercise their sexual and reproductive health and rights. This $18.2-million project seeks to address negative social norms and attitudes that hinder women and girls’ decisions and control over their bodies and strengthen the health system to improve access to sexual and reproductive health services, particularly in conflict-affected and disadvantaged regions of the Philippines. Since 2018, nearly 350 health workers have been trained by this project to deliver gender-responsive sexual and reproductive health services, including family planning. In 2022 alone, these trained health workers reported that they provided family planning services, including modern methods of contraception, to over 61,000 women of reproductive age across 21 municipalities.
SRHR advocacy
In 2021-2022, many Canadian stakeholders raised concerns about the rise in misinformation and disinformation and the backlash to women’s rights and SRHR that they were observing in global, regional and country-level fora. For example, anti-rights activists in many countries continued to promote the Geneva Consensus Declaration, which encourages governments to remove existing protections around access to safe abortion and post-abortion care and SRHR for women and girls. Through coordinated efforts with other like-minded donors, we worked to counter this effort by participating in joint demarches (for example, in the Democratic Republic of Congo) to dispel misinformation and to provide factual information about the Geneva Consensus Declaration to government officials.
At the 10YC project level, we also financed several projects that support SRHR advocacy, including:
- The Empowering Women and Girls in Ethiopia project implemented by Ethiopaid increased women and girls’ access to and knowledge of their SRHR. In 2021-2022, over 47,000 community members received training on literacy, reproductive health, family planning and harmful traditional practices, as well as on nutrition and immunization. Additionally, over 6,600 men and boys were sensitized to understand gender issues and share unpaid care burdens through events, advocacy activities and community mobilization. Also, 22 women’s associations made up of 314 members (309 women) were trained to improve awareness of SRHR and prevention of gender-based violence.
- The Integrated Management of Maternal and Child Health in Artibonite (PRISMA II, Prise en charge intégrée de la santé de la mère et de l'enfant dans l'Artibonite) project in Haiti, implemented by Centre for International Cooperation in Health and Development educated boys and men about positive masculinity, sexual and reproductive health and gender-based violence. In 2021-2022, over 8,600 boys and men were reached, for a total of nearly 15,000 since the project began. The project trained groups of men as peer educators, who will in turn train their peers to form a critical mass of men who are sensitive to the needs of their wives and committed to the overall principles of respect for women’s rights. In addition, in 2021-2022, over 1,400 men stood with women to denounce gender-based violence and promote gender equality, including during the commemoration of the International Day for the Elimination of Gender-Based Violence.
Project spotlight: Testimonial from Enhancing sexual and reproductive health for women of reproductive age in Northern Nigeria (Clinton Health Access Initiative)
Hadiza Umar is a trained midwife working at Warawa Primary Health Centre and an active adolescent and youth-friendly service provider. She has been providing family planning, antenatal, and labour and delivery services. “At first, I believed that unmarried adolescents should not be given contraceptives. However, with the training I received, I realized that we have been wrong for a very long time; we need to draw them closer, provide proper counselling and appropriate services to adolescents. After the training, I began to encourage adolescents to use the different family planning methods, and they have been coming for both contraceptives and counselling. The adolescents have learned to open up to us at the clinic and share their concerns, and we have been able to help them. Health care workers should not turn their backs on adolescents who are interested in learning more about contraceptives to prevent unplanned pregnancy and use condoms to prevent sexually transmitted diseases.”
Prevention of and response to sexual and gender-based violence
The COVID-19 pandemic has exacerbated existing gender inequalities and the vulnerabilities of women and girls. Lockdown and related mitigation measures—such as isolation and quarantine measures, school closures and restricted access to health and social protection services—have increased SGBV and limited women and girls’ ability to make choices about their own bodily autonomy. Using an intersectional feminist approach, our international assistance response to COVID-19 prioritized action to address the gendered impacts of the pandemic and to target the most marginalized, particularly by supporting local organizations working on the front lines. Central to this response are our efforts to address the increase in SGBV caused by the pandemic and to ensure access to essential health services, including SRHR. Based on the 2021-2022 data, we were able to reach over 42 million people through projects that help prevent, respond to and end SGBV, including child, early and forced marriage and female genital mutilation.
Our long-term institutional support to multilateral organizations, the United Nations (UN) and other partners also contributed to the prevention of SGBV in 2020-2021. For example, UNDP supported over 5,300 community-based organizations to combat both the pandemic and its “shadows” of domestic violence and human rights abuses, including racism and xenophobia. During the Generation Equality Forum’s opening ceremony in Paris on June 30, 2021, we announced $10 million of emergency support for the UNFPA-UNICEF Global Programme to End Child Marriage to help ensure sustained progress toward ending child marriage despite school closures, disruptions to programs and the increase in SGBV caused by the COVID-19 pandemic. This emergency support helped 865 schools provide quality, safe and gender-friendly education. In addition, it helped close to 16 million community members participate in dialogues and learning sessions about gender equality, alternatives to child marriage, the rights of adolescent girls and the importance of addressing harmful masculinities. Through these contributions, we joined the Generation Equality Forum’s Action Coalition on Gender-Based Violence as a commitment maker.
We have provided a total contribution of $14 million to the UN Trust Fund to End Violence against Women for the period 2019 to 2022, which includes $12 million in additional COVID-19 funding. Our commitment to the Trust Fund’s COVID response supported the core capacity of its existing grantees, primarily women’s rights organizations, to respond to the increase in SGBV and provide comprehensive services to survivors of violence. In 2021-2022, the Trust Fund’s grantees reached over 261,000 women and girls in 68 countries and territories. This included over 66,000 women and girls who used specialist support services to end and prevent SGBV and allowed nearly 20,000 women and girls to access free legal aid related to SGBV.
Nutrition
Nutrition is a critical part of health and development and a maker and marker of sustainable development with direct and indirect links to all the SDGs. In 2021, more than 3.1 billion people in the world (42%) were unable to afford a healthy diet due to COVID-19 disruptions and climate change, with food insecurity disproportionately affecting women and people living in rural areas. Between 691 and 783 million people in the world faced hunger in 2022, with almost 600 million people projected to be chronically undernourished in 2030. We remain concerned that the gender nutrition gap continues to worsen globally, as women and girls often eat least and last.
Our funding for nutrition is a key component of the 10YC and supports Canada’s 2021 Nutrition for Growth (N4G) financial and policy commitments.
We take a “twin-track” approach to food security and nutrition, supporting targeted policy, programming and advocacy efforts with the greatest potential. This includes direct action to immediately tackle malnutrition and micronutrient deficiencies among those experiencing vulnerability and marginalization, alongside long-term nutrition-sensitive interventions that address the root causes of malnutrition and poverty.
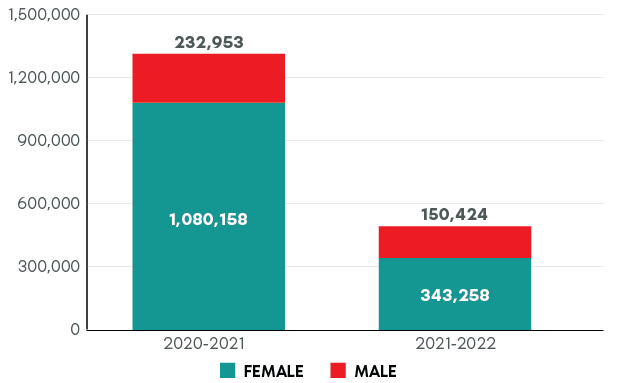
KPI data spotlight: People reached with community-based nutrition services and programs
In 2021-2022, KPI data shows that our nutrition projects reached over 490,000 people.
This represents a decrease from 2020-2021 partly as a result of 3 large Partnership for Maternal Newborn and Child Health nutrition projects closing in 2021-2022. New GAC-funded nutrition projects have been initiated and will be included in future 10YC reporting.
Figure 11: KPI data: People reached with community-based nutrition services and programs
Text version
- Male 2020-2021: 232,953
- Female 2020-2021: 1,080,158
- Male 2021-2022: 150,424
- Female 2021-2022: 343,258
Another factor contributing to the decrease is that many of our nutrition projects shifted the focus of their activities to assisting with the COVID-19 response. As a result, the number of health care workers trained increased to over 159,400 from 79,000 in 2020-2021. The number of health facilities supported also increased to nearly 1,400 health facilities from 127 in 2020-2021.
Nutrition International (NI) is a global organization based in Ottawa and Canada’s main partner in nutrition programming. It is the leading organization in micronutrient supplementation worldwide. In 2021-2022, our support helped NI reach nearly 490 million people with their salt iodization programs. Their weekly iron and folic acid programs reached 1 million adolescent girls, more than doubling the indirect reach from the previous year due to pandemic response funds.
Since 1998, we have been the largest donor to vitamin A supplementation (VAS) programs worldwide through our institutional support to Nutrition International and targeted vitamin A programming with UNICEF. Rates of vitamin A supplementation fell sharply due to the pandemic in 2020. As a result of our additional funding during the COVID-19 response, in 2021-2022, NI and UNICEF reached 167 million children with 2 doses of vitamin A. This represented an increase of 68 million children from the previous year.
Project spotlight: Nutrition International (NI) support to adolescent nutrition
NI works with teachers and health workers to deliver weekly iron and folic acid supplements and nutrition information to over 2 million adolescent girls in 8 countries: Indonesia, Pakistan, India, Bangladesh, Kenya, Ethiopia, Senegal and Tanzania. In 2021-2022 alone, these programs averted 137,000 cases of anaemia among adolescent girls who, as a result, are more likely to stay in school and succeed in their studies. Working mainly through schools, these programs build agency and self-confidence among adolescent girls who assume leadership roles to improve nutrition and combat taboos on important issues like menstrual hygiene management in their schools and communities. These programs also actively involve adolescent boys, making them more likely to challenge traditional gender roles and to prioritize health and nutrition for their future wives and children, particularly during pregnancy. Better health and school outcomes for adolescent girls improve self-sufficiency and lifetime earnings, contributing to the overall economic growth of their communities and countries.
Another key nutrition partner for Canada in 2021-2022 was World Vision Canada. Their Enhancing Nutrition Services to Improve Maternal and Child Health in Africa and Asia (ENRICH) project (2016 to 2021) contributed to the reduction of maternal and child mortality by delivering gender responsive essential MNCH and SRHR services, increasing the production, consumption and utilization of nutritious foods and micronutrient supplements during the first 1,000 days of life. In 2021-2022, over 20,000 families with children aged 6 to 24 months were provided with micronutrient powders (MNPs). The MNPs served as point-of-use fortification of children’s meals with micronutrients essential for their health and growth. ENRICH worked with consortium partner HarvestPlus and national agricultural technical agencies to promote the uptake of biofortified crops by local farmers and their inclusion in the diets of women and children. For instance, partnerships between the ENRICH Kenya team, HarvestPlus, the Kenya Agriculture and Livestock Research Organization (KALRO), the Kenya Plant Health Inspectorate Services and a local seed company led to the production and distribution of 70 metric tonnes of high-iron bean seeds, reaching close to 23,000 households with children under 2 years of age in Kenya over the 5 years of the project.
In 2021-2022, GAC support to HarvestPlus also reached over 790,000 women across 6 countries with iron and vitamin A-fortified foods, in addition to providing over 875,000 farm households (60% headed by women) with seeds fortified with zinc, vitamin A and iron.
Policy and advocacy
Global health
We continued to advance the 10YC policy objectives through active engagement at global fora, such as the World Health Assembly, the G7/G20 and the UN. We also continued to advocate with key international, regional and national stakeholders.
Key advocacy moments in 2021-2022 included the following:
- We participated in the historic World Health Assembly Special Session (November 29 to December 1, 2021), when WHO Member States adopted a decision to set up an intergovernmental negotiating body to develop and negotiate a WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response (PPR), which will serve to enhance collective action and accountability to address gaps and strengthen international collaboration on pandemic PPR.
- We successfully negotiated progressive language reaffirming G7 countries’ commitment to SRHR of all persons and G20 countries’ recognition of the importance of ensuring the continuity of health services, including for sexual and reproductive health, in light of constrained access during the pandemic.
Spotlight on Canada’s global health and SRHR leadership
We participated in the 6th International Conference on Family Planning (ICFP), held in Pattaya, Thailand, from November 14 to 17, 2022. The conference theme was “Family Planning and Universal Health Coverage: Innovate. Collaborate. Accelerate.” As a SheDecides Champion, Canada’s Minister of International Development delivered recorded remarks at the opening ceremony to demonstrate Canada’s continued leadership and championing of women’s rights and bodily autonomy, in particular a women’s right to safe abortion. The ICPF brought together approximately 5,000 delegates in a hybrid format.
Comprehensive SRHR
We work to advance SRHR advocacy with global partners and initiatives like SheDecides, UNFPA, the Global Safe Abortion Dialogue, the GFF, the GFATM and Family Planning 2030 (FP2030).
Key advocacy moments in 2021-2022 included the following:
- To commemorate the International Day of Youth in August 2021, Canada co-hosted an intergenerational roundtable on access to CSE in the Americas and Caribbean with the International Planned Parenthood Federation. The Minister of International Development spoke alongside Jamaica’s Minister of Youth and representatives from UNESCO, Colombia’s Ministry of Education, and youth activists from the region to advocate for the integration of CSE into policies that reach youth in and out of school.
- The Minister of International Development delivered Canada’s address at the United Nations General Assembly High-Level Meeting on AIDS in June 2021. The event reviewed the progress made since 2016 in preventing and reducing the impact of HIV. UN member states agreed on a political declaration outlining what is to be achieved by 2026. The Minister also chaired a panel entitled Advancing Gender Equality and Empowering Women and Girls in the AIDS Response.
Gender-sensitive nutrition
We continue to advocate for the integration of nutrition across programs in health, education and agriculture, with a cross-cutting focus on gender equality. Our nutrition advocacy partnerships include those with the World Food Programme in support of nutritious school meals, and with the Global Nutrition Report and Standing Together for Nutrition in support of relevant research.
Key advocacy moments in 2021-2022 included the following:
- Canada participated actively in the 54th UN Commission on Population and Development (CPD, April 19 to 23, 2021), which focused on the theme of “Population, food security, nutrition and sustainable development.” Member States successfully adopted a resolution on this theme, marking the first time a consensus outcome was achieved at CPD since 2016.
- The Minister of International Development participated in the December 2021 Tokyo Nutrition for Growth (N4G) Summit, the culmination event of the N4G 2021 Year of Action. He announced $195 million in support for global nutrition efforts and continued to champion the need for a comprehensive approach to malnutrition, focusing both on low-cost, high-impact interventions to address acute malnutrition and on longer-term work to address the underlying determinants of malnutrition. The announcement built on the momentum generated by the December 2020 kick-off event for the N4G Year of Action, which we co-hosted with Bangladesh. The event mobilized over $3 billion in global nutrition programming, including our N4G pledge of $520 million in nutrition-specific programming over 5 years. A portion of the 2021 announcement contributes to the $520-million pledge.
COVID-19 response and recovery
In 2021-2022, we continued to be a leading donor to the global COVID-19 response and a vocal champion for vaccine equity.
Key advocacy moments in 2021-2022 included the following:
- Prime Minister Trudeau participated live during the first session of the Global COVID-19 Summit hosted and chaired by U.S. President Biden on September 22, 2021. He emphasized the importance of mass immunization in stopping the spread of COVID-19 and unlocking global economic recovery and reaffirmed our commitment to strengthening global health security to prevent and prepare for future pandemics. Both the Minister of Foreign Affairs and the Minister of International Development participated actively in subsequent U.S.-led COVID-19 Ministerial meetings.
- Prime Minister Trudeau participated virtually in the Global Health Summit co-hosted by the European Commission and the Italian G20 Presidency in May 2021. The Prime Minister and other leaders of G20 and invited countries and international organizations shared COVID-19 lessons learned and endorsed the Rome Declaration of principles. These principles are to guide immediate actions to end the pandemic as well as future cooperation to prevent and better prepare for health emergencies.
- The Minister of International Development participated in the COVAX Advanced Market Commitment (AMC) “One World Protected” Summit hosted by Japan in June 2021.She announced our pledge of $220 million to the COVAX Facility. Alongside Ministers from Indonesia and Ethiopia, our Minister of International Development also co-hosted meetings of the COVAX AMC Engagement Group in May 2021, July 2021, October 2021 and March 2022.
V. COVID-19 response and recovery
Our overall global health spending for 2021-2022 includes investments to address the COVID-19 pandemic. In 2020-2021 and 2021-2022, GAC received additional one-time funding for COVID-19 programming that is not included in the 10YC financial tracking methodology. However, it is a key component of our leadership work on global health and had a significant impact on the global health landscape in 2021-2022.
The emergence of COVID-19 has underscored the need to reinforce and deliver on joint commitments by the international community to strengthen health systems and reinforce prevention, detection, emergency planning and preparedness capabilities worldwide. We are committed to working with other countries and global health partners to act on the lessons learned from COVID-19.
Global COVID-19 response through the ACT-Accelerator
The Access to COVID-19 Tools (ACT)-Accelerator represented an unprecedented level of engagement and investment for our international assistance program. During 2021-2022, we played a leadership role in this global effort with Ministerial engagement:
- on the ACT-Accelerator’s Facilitation Council
- at the ACT-Accelerator’s resource mobilization kick-off event (February 2022)
- as co-chair of the ACT-Accelerator Vaccine Pillar (COVAX) Advance Market Commitment (AMC) Engagement Group, the arm of COVAX helping 92 low and lower-middle income countries to have equitable access to vaccines
We were also a leading financial contributor to the ACT-Accelerator, committing over $1.3 billion in new resources for ACT-Accelerator partners from the start of the pandemic to March 2022. These investments in the ACT-Accelerator contributed to increasing developing countries’ access to COVID-19 tests, treatments and vaccines, which will continue throughout 2022 and into 2023.
In collaboration with others, Canada’s support to partners of the ACT-Accelerator has enabled the achievement of significant results, including the following:
- Shipment of over 1.4 billion doses of vaccines to 145 countries and territories via the COVAX Facility, of which over 1.2 billion have gone to the AMC’s low and lower-middle income participants.
- Supporting research and development, which enabled access to a portfolio of 14 vaccines/candidates across multiple technology platforms.
- Procurement of over 158.3 million COVID-19 tests for lower income countries (LICs) and lower-middle income countries (LMICs) and over 30.4 million dexamethasone tablets delivered to 47 countries.
- More than 120 countries received technical and operational support from the WHO and UNICEF in utilizing oxygen plants, concentrators, cylinders and other vital infrastructure, and approximately 70 LICs and LMICs received funding of $560 million from the Global Fund’s COVID-19 Response Mechanism program for the procurement and use of oxygen supplies.
- Development of the first Oxygen Plant System (Plant-in-a-Box), which produces large volumes of medical-grade oxygen for patients in low-resource settings. With Canada’s support, UNICEF has procured 44 Oxygen Plant-in-a-Box packages for 30 countries.
We provided $100 million to the World Health Organization for the implementation of the Health Systems and Response Connector of the Access to COVID-19 Tools Accelerator. This funding supported a total of 73 countries to help identify and address health system bottlenecks for the effective delivery of COVID-19 tools.
Pandemic prevention, preparedness and response
Several lessons have emerged from COVID-19, and we are committed to applying these lessons moving forward. Firstly, the global community must work to preserve gains made and help mitigate further backsliding of Sustainable Development Goal progress by ensuring consistent funding, both during and after the pandemic. Our 10YC has contributed to this effort by providing consistent funding for essential health services, including SRHR, throughout the pandemic.
Secondly, key COVID-19 review bodies, including the Independent Panel for Pandemic Preparedness and Response and the G20 High Level Independent Panel on Financing the Global Commons for Pandemic Preparedness and Response, released their respective reports in 2021 and made important recommendations on strengthening pandemic PPR. We continue to engage in multilateral discussions on this, including within the G7, G20, WHO and United Nations General Assembly. We will continue to work to ensure that Canadian priorities are reflected in these fora.
VI. Transparency, engagement and learning
As part of the Accountability Framework for the 10YC, the Canadian government has committed to unprecedented transparency and accountability to stakeholders. Through the 10YC annual report and annual stakeholder workshop, we are making reliable information on the 10YC available and engaging with stakeholders and the Canadian public on how to increase our impact on global health outcomes.
Building internal capacity
In 2020-2021, Global Affairs Canada (GAC) continued to build internal capacity to deliver on the 10YC and ensure that we are accurately capturing the programming that we are undertaking. Regular learning sessions for staff were held on:
- project coding for the 10YC
- 10YC key performance indicator training
- SRHR programming, including development and dissemination of SRHR neglected areas programming guidance notes
First annual stakeholder engagement event in February 2023
The objective of this event was to review progress on the first year of implementation of the 10YC (2020-2021) and discuss challenges and opportunities for 10YC implementation. The in-person event brought together approximately 50 executive and managerial-level representatives of Canadian CSO partners in global health, including SRHR partners, as well as GAC officials from across several branches.
Participants identified areas where GAC and Canadian CSOs could work together to further advance the 10YC, including:
- deepened collaboration on health systems strengthening (HSS) between GAC and Canadian CSOs, given the HSS expertise residing in Canadian organizations
- continued learning exchanges between GAC and partners on monitoring and evaluation to collectively tell the 10YC results story
- increased collaboration between GAC and stakeholders to find entry points to work with and support women and youth advocates at the grassroots level
- better utilization of research to inform programming for more evidence-based approaches to global health programming and better understanding of contexts
Publicly available information on Canada’s global health spending
- Canada’s Canada’s International Assistance Data is a mandated annual report to Parliament under the Official Development Assistance Accountability Act. This report provides a single source for international assistance expenditure statistics for Canada as a whole, including official development assistance and other official assistance.
- The OpenGAC website provides access to GAC data and information, including on our international assistance, and more.
- The GAC Project Browser is an interactive tool that allows you to search GAC’s international projects and download information as open data files.
- The Government of Canada’s 10YC webpage is updated with new and developing information to encourage transparency and accountability with the public and the community on the 10YC.
VII. Looking forward
The 10-year commitment is ambitious in scope, scale ($1.4 billion annually) and length (until 2030), demonstrating our ongoing leadership in global health. As this report demonstrates, we are on track in scaling up investments to meet the target of an average of $1.4 billion annually by 2023-2024, with $700 million per year invested in SRHR by 2023-2024 and increasing annual investments in the SRHR neglected areas.
To achieve these objectives, we will continue to play a leadership and advocacy role on the global stage. We will advance our global health and nutrition priorities through active engagement in multilateral fora, such as the G7/G20 and the UN, where Canada will advocate for strong SRHR and gender equality commitments. We will also continue our advocacy efforts among key international, regional and national stakeholders.
As always, women and girls are at the centre of everything we do. In the context of increasing global pushback against women’s rights and bodily autonomy, we will continue to scale up support for and prioritize programming in the SRHR neglected areas, including by partnering with Canadian health partners to improve the quality of and access to integrated health services for women, adolescents and children.
Internally, GAC will continue to raise awareness about the 10YC among staff at all levels, with a focus on the SRHR neglected areas. This will be done in part by continuing to invest in tools and training, including coding guidance, which will enable programs to be effective and impactful. This will also help ensure that investments in global health and SRHR are scaled up while also managing competing pressures.
We are as committed as ever to transparency and accountability toward our stakeholders and will continue to communicate progress on the 10YC through the publication of annual reports, which are a key part of the Accountability Framework for the 10YC. In addition, the contents of this report will be discussed with stakeholders at the second annual stakeholder event in the fall of 2023, providing another valuable engagement opportunity to discuss progress, challenges and opportunities in the implementation of this commitment.
As the world moves toward recovery from the COVID-19 pandemic and toward prevention, preparedness and response to future health emergencies, we will continue to work with our partners and the global community at large to preserve the gains made and mitigate further backsliding of Sustainable Development Goal progress by ensuring consistent funding, both during and after the pandemic. This will include a renewed focus on strengthening equitable and resilient health systems that serve as the foundation for essential health services and act as the first line of defence against future pandemics.
Annex I – Adjusted 2020-2021 spending totals
Following adjustments to the methodology, the 2020-2021 spending totals now includes IDRC and prevention of and response to sexual and gender-based violence (SGBV) in the neglected areas. Updated figures from the 2020-2021 report are:
- Total 10YC spending: $1.25 billion
- SRHR spending: $495.9 million
- Neglected area spending: $170.9 million
- Safe abortion and post-abortion care: $1.89 million
- Comprehensive sexuality education: $5.36 million
- Family planning and contraception: $49.46 million
- SRHR advocacy: $47.3 million
- Prevention of and response to SGBV: $66.86 million
Annex II – Key multilateral results
This annex provides additional information on results achieved through key multilateral partnerships.
United Nations Population Fund (UNFPA): During the Annual Session of the UNFPA Executive Board 2021, UNFPA partially achieved the desired outputs on (a) the development of sexual and reproductive health policies prioritizing furthest behind populations and (b) the delivery of sexual and reproductive health commodities. Due to the pandemic, several countries could not prioritize the policy and system development indicators relating to supply management strategies and sexual and reproductive health action plans.
United Nations Children’s Fund (UNICEF): UNICEF has achieved significant progress in various areas of global well-being and sustainable development, benefiting millions of children and adolescents worldwide. Our support to UNICEF has contributed to the provision of essential services to approximately 336 million children, prevention of malnutrition, provision of education for out-of-school children and support to skill development programs across 91 countries. Amid the COVID-19 pandemic, UNICEF’s role as the COVAX Facility’s procurement coordinator has been vital, leading to the distribution of 958 million COVID-19 vaccines to 144 countries and ensuring equitable access to vaccines worldwide.
Gavi, the Vaccine Alliance (Gavi): We provided dedicated funding and advocated for better coordination, services and support for in-country delivery and distribution of vaccines for the poorest and most vulnerable. In December 2021, with Canada’s support as a member, the Board created the COVID-19 Vaccination Delivery Support Temporary Steering Committee, the oversight body for the COVID-19 Vaccine Delivery Partnership (CoVDP). The CoVDP has been key in providing additional and focused support to countries lagging on COVID-19 vaccination and countries dealing with significant humanitarian contexts. To ensure that critical CSO voices were heard and involved in equitable vaccine delivery funding, Canada was also a strong advocate for Gavi’s new Civil Society and Community Engagement Approach, which was approved by the Board. Importantly, the new approach recognizes the competitive advantage of CSOs in addressing gender barriers to vaccination, a strategic priority for Canada, and reaching missed children and communities, particularly in fragile and conflict-affected settings outside government reach. Canada was also instrumental in working with Gavi to develop a strategy to launch and introduce HPV vaccination by providing an earmarked contribution over the period of our funding.
Global Financing Facility for Women, Child and Adolescent Health (GFF): As a GFF Board member, we continued to promote gender equality and SRHR as a key priority for the GFF. We played an influential role in the development of the GFF’s Institutional Strategy for 2021 to 2025, advocating for gender equity to be at the core of the strategy and SRHR to be a critical component. We also advocated for the GFF to take a stronger public position in support of SRHR, which led to the launch of the GFF’s SRHR Acceleration Plan at the Generation Equality Forum in 2021. We were a strong advocate for the inclusion of the GFF in the Access to COVID-19 Tools Accelerator (ACT-A) in 2021, given the GFF’s expertise on women, child and adolescent health and ability to shine a light on the disproportionate impact of the pandemic on women and children. In 2021-2022, we provided $50 million under ACT-A to support the GFF’s COVID-19 EHS grants. This funding helped the GFF to provide $292 million in EHS grants to 18 countries in 2021-2022.
Canada also co-hosted the GFF’s 2021-2022 Resource Mobilization campaign, which generated $570 million. In this role, we helped to raise the profile of the GFF’s work and ensure the GFF could continue to deliver on its core mandate while responding to emerging needs resulting from COVID-19. We also served as co-chair of the GFF’s multi-sectoral Investors Group from 2020 to 2022, where we were able to effectively advocate for a strong equity focus and enhanced aggregate reporting.
Global Fund to Fight Aids, Tuberculosis and Malaria (Global Fund): Through our role on the Board of the Global Fund, in 2021-2022, we were instrumental in ensuring that health equity, gender equality and human rights were embedded in the Global Fund’s new 2023 to 2028 Strategy. As a result of our strong engagement and of like-minded Board members through Board and Committee sessions, the 2023 to 2028 Strategy was approved by the Board with a new strategic objective of maximizing health equity, gender equality and human rights, and with new emphasis on resilient and sustainable systems for health as a key foundation for universal health coverage.
Global Polio Eradication Initiative (GPEI): As a sovereign donor representative on the Polio Oversight Board, we worked with the GPEI and other donors to maximize the effectiveness of its governance and strengthen accountability for program implementation. Canada made sure that gender equality remained high on the program’s agenda. As a result, the GPEI took decisive steps forward to strengthen gender mainstreaming across the program, including establishing a Gender Mainstreaming Group, introducing gender-specific key performance indicators, and ensuring a dedicated budget was in place for gender mainstreaming activities. We also reinforced the importance of further integrating polio eradication into a broader suite of health services to make the most of limited resources and increase uptake in vaccine-weary contexts. This resulted in more deliberate partnering with essential immunization services and coordination with broader health, humanitarian and sanitation sectors.
- Date modified: